什麼是鼻竇增高術?適合族群、手術流程、風險與費用

前言
鼻竇增高術後遺症、鼻竇增高術失敗是許多植牙患者擔心的事情,有關鼻竇增高術ptt版上也能看到很多相關的討論和疑問,甚至出現一些相關的迷思,關於鼻竇增高術費用更是讓人看的眼花撩亂。以下讓我們大叔來一一解答,希望對即將植牙的患者有些幫助。

鼻竇在哪?
鼻竇是位在頭部內部的數個空腔,分成四對,其中和植牙比較有關係的是上顎竇,也是今天鼻竇增高術的主角。上顎竇所在的位置,在全景X光片中大概位於後牙區,一般來說是第二小臼齒後面的區域,所以在上顎後牙區的植牙才會有機會遇到鼻竇增高術。

我的鼻竇發生了什麼事?為什麼需要鼻竇增高術?
你可能會好奇,對,我知道鼻竇,但我是要植牙,關鼻竇什麼事?人類是個奇怪的東西,一但知道某些沒在用之後,他就會開始跟你耍廢,所以你可能聽過被拔掉牙齒的牙齦會萎縮。
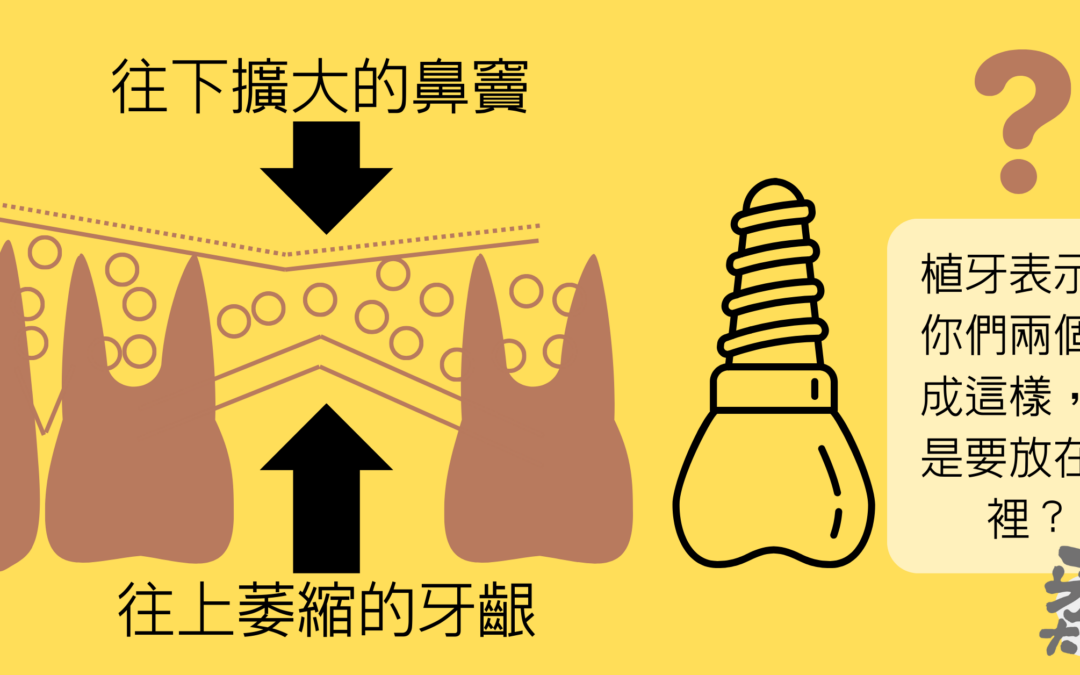
在上顎後牙區,沒牙齒的牙齦不但會萎縮,在缺牙處上方的上顎竇還會氣室化,越變越低使得可用骨頭越來越少。你的上顎齒槽骨就像是一片夾心餅乾,不但牙齦會往上萎縮外,上面的鼻竇也會往下變大,兩者擠壓下讓中間可供植牙的齒槽骨越變越少。

上顎後牙區,植牙需要的齒槽骨高度一般建議至少要有8mm以上,齒槽骨高度不足時,就需要鼻竇增高術,讓植體周圍可以有骨頭。

鼻竇增高術的後遺症?
鼻竇增高術的術式
鼻竇增高術的術式通常分為兩種,一種是利用植體要植入的位置提升鼻竇,一種是從鼻竇側面開窗提升鼻竇。第一種的傷口較小,通常可以在植牙當下一起補骨,適用於齒槽骨吸收不是那麼嚴重的狀況,植牙區齒槽骨高度通常還有3-4mm以上。
第二種側面開窗的方式,傷口較大,一般需要先補完骨頭之後待一段時間才會再安排植牙手術,適用於齒槽骨吸收很嚴重的患者,植牙區齒槽骨高度通常只剩下1-2mm。
鼻竇增高術後遺症
一般來說,鼻竇增高術後遺症並不明顯,沒有太多不適。術後的兩週內可能會有手術區域腫脹、微出血、或發炎的狀況,屬於手術後的正常情形,其中側開窗鼻竇增高術的不適感會略大於植體位置的鼻竇增高術。配合一些傷口的照護措施,例如冰敷、服藥、二極體低能量雷射傷口照護、高壓氧艙,都可以減緩不是,增快傷口的恢復。
鼻竇增高術的禁忌症
鼻竇增高術的禁忌症跟一般植牙手術禁忌症相同:糖尿病、高血壓、抽菸、凝血功能不佳者,除此之外比較需要注意的則是如有感冒,尤其有鼻竇發炎、流鼻水、黃鼻涕、打噴嚏的症狀的話會建議將手術日期延後。
鼻竇增高術的費用
鼻竇增高術的費用,在臺南市牙醫師公會建議收費裡是一區5萬,一般來說大概介於1.5萬~5萬之間,視手術困難度、區域大小、骨粉所需多寡來決定。
不想做鼻竇增高術,有沒有其他的選擇?
醫師啊,我就不想手術啊,那有其他選擇嗎?
選擇一
如果你的上顎後牙缺牙區,前後都還有牙齒,植牙外的另一個選擇就是做傳統的牙橋。
選擇二
假如你還是想植牙,而且齒槽骨高度也沒有到太糟糕,介於6-8mm之間,那是有機會使用短植體,目前最短植體的長度是6mm,也就是說6mm以上的齒槽骨高度有機會可以不用作鼻竇增高術。
- 你可能想知道:缺牙不想植牙?你還有牙橋這個選擇:牙橋禁忌與適應症
- 你可能想知道:缺牙影響外觀,但植牙好嗎?植牙4大好處與3缺點
- 你可能想知道:快速搞懂那些植牙名詞:微創植牙、植牙補骨補皮、即拔即植、導板植牙
總結
植牙區齒槽骨高度>3mm,植牙和鼻竇增高術有機會可以一起做,少一次手術,手術範圍較小。
植牙區齒槽骨高度1~2mm,側開窗方式進行鼻竇增高,手術範圍較大,手術後一段時間才能安排植牙手術。
不想做鼻竇增高術:1.前後有牙,牙橋,2.齒槽骨高度>6mm,短植體。
『植體周圍維持一定的骨頭量,對於植體來說是很重要的一個保護,所以如果真的上顎後牙植牙區齒槽骨高度不足,鼻竇增高術這一步千萬不能跳過,對於植體日後的使用壽命是有很大的影響的。』
Preface
Sinus Lift Surgery Complications and Sinus Lift Surgery Failure are concerns for many dental implant patients. There are many discussions and questions about sinus lift surgery , and even some myths have arisen. The cost of sinus lift surgery is also a confusing topic. Let’s address these issues one by one to hopefully provide some assistance to patients preparing for dental implants.

Where are the sinuses?
The sinuses are several air-filled cavities located within the head. There are four pairs of sinuses, but the maxillary sinuses, which are related to dental implants, are the focus of today’s discussion. The maxillary sinuses are typically located behind the posterior teeth area, approximately behind the second molar. Therefore, sinus lift surgery may be necessary for dental implants in the posterior maxilla.

What happens to my sinuses? Why is sinus lift surgery necessary?
You might wonder why sinuses are relevant when you’re getting dental implants. Humans are peculiar creatures; once something is not in use, it starts to deteriorate. So, you may have heard that the gums recede after teeth are extracted.
In the posterior maxilla, where there are no teeth, the gums not only recede but the maxillary sinus above the edentulous area pneumatizes, gradually lowering and reducing the available bone. Think of your maxillary bone as a sandwich cookie; not only does the gum recede upward, but the sinus above also expands downward, reducing the available bone for implant placement.

For dental implant placement in the posterior maxilla, it’s generally recommended to have a bone height of at least 8mm. If the bone height is insufficient, sinus lift surgery is necessary to provide adequate bone around the implant.

What are the complications of sinus lift surgery?
Types of sinus lift surgery
Sinus lift surgery typically comes in two types: one involves lifting the sinus using the area where the implant will be placed, and the other involves lateral window access to lift the sinus.
The first type involves a smaller incision and can usually be performed concurrently with implant placement, suitable for cases where bone resorption is not severe, and there is still 3-4mm of bone height in the implant area.
The second type, lateral window access, involves a larger incision and generally requires bone grafting before implant placement. This method is suitable for patients with severe bone resorption, where only 1-2mm of bone height remains.
Complications of sinus lift surgery
Generally, complications after sinus lift surgery are not significant and involve minimal discomfort. Swelling, minor bleeding, or inflammation in the surgical area may occur within the first two weeks post-surgery, which is normal. However, discomfort may be slightly greater with lateral window sinus lift surgery compared to lifting the sinus using the implant site. Proper wound care measures such as ice packs, medication, low-level laser therapy, and hyperbaric oxygen therapy can alleviate discomfort and promote faster healing.
Can sinus lift surgery fail?
Possibility 1: Sinus membrane perforation
Sinus lift surgery, like any surgical procedure, carries the risk of failure. The primary reason for sinus lift surgery failure is perforation of the sinus membrane during the procedure. The thickness of each individual’s sinus membrane varies, making the surgery more challenging when the membrane is too thick or too thin, increasing the risk of perforation.
Although perforation can occur, there’s no need to panic. If the perforation is small, the torn sinus membrane can be sutured or avoided using surgical techniques, and reinforcement with a membrane can still allow the surgery to be successful. If the perforation is extensive and bone grafting cannot be completed during the same surgery, the flap will be sutured, and a waiting period will be necessary for the perforation to heal before proceeding with further surgery.
Possibility 2: Inadequate bone growth after grafting
Another reason for failure is inadequate bone growth after grafting. After surgery, the bone graft undergoes a conversion process to become natural bone, which may result in less bone formation than expected. If bone formation is inadequate, additional bone grafting may be required during implant placement. This situation is more likely to occur with lateral window sinus lift surgery, but with minimal bone grafting required during secondary bone grafting, it can be managed concurrently with implant placement, reducing the number of surgeries needed and minimizing concerns.
Contraindications for sinus lift surgery
The contraindications for sinus lift surgery are similar to those for general dental implant surgery: diabetes, hypertension, smoking, and impaired clotting function. Additionally, it’s essential to avoid sinus lift surgery during cold or sinus infections, especially if symptoms such as sinus inflammation, nasal discharge, yellow nasal mucus, or sneezing are present; in such cases, surgery should be postponed.
Cost of sinus lift surgery
The cost of sinus lift surgery, according to the Tainan Dental Association, typically ranges from 15,000 to 50,000 NT dollars, depending on the complexity of the surgery, the size of the area, and the amount of bone graft needed.
Alternatives to sinus lift surgery
If you prefer to avoid surgery, there are other options:
Option 1
If you have teeth both anterior and posterior to the edentulous area, traditional bridges are an alternative to implants.
Option 2
If you still want implants and the bone height is not severely compromised, ranging between 6-8mm, short implants may be an option. Currently, the shortest implants available are 6mm in length, meaning that bone heights above 6mm may not require sinus lift surgery.
Conclusion
For implant sites with bone height >3mm, sinus lift surgery may be performed concurrently with implant placement, reducing the surgical area and minimizing discomfort.
For bone heights between 1-2mm, lateral window sinus lift surgery is necessary, involving a larger surgical area and a waiting period before implant placement.
If you prefer to avoid sinus lift surgery: 1. If adjacent teeth are present, consider traditional bridges; 2. If bone height is >6mm, short implants may be an option.
“Maintaining a certain amount of bone around implants is crucial for their long-term success. Therefore, if bone height in the posterior maxilla is insufficient, sinus lift surgery should not be skipped, as it greatly impacts the longevity of implants.”